
If you’re navigating a PCOS diagnosis, the term ‘ovarian cysts’ can feel both confusing and concerning. You might be wondering what they are, if they’re dangerous, and what your doctor is actually looking for during an ultrasound. The evaluation and monitoring of ovarian cysts in PCOS is a nuanced process, distinct from how other ovarian conditions are managed. It’s less about finding a single, problematic cyst and more about understanding the overall pattern of your ovarian function.
Endocrinologists, specialists in hormone-related conditions, approach this with a specific lens. Their goal isn’t just to take a picture; it’s to interpret what the structure of your ovaries reveals about the underlying hormonal environment. This careful assessment forms a cornerstone of the diagnosis and helps guide a personalized, long-term management plan.
What are they actually looking for on an ultrasound?
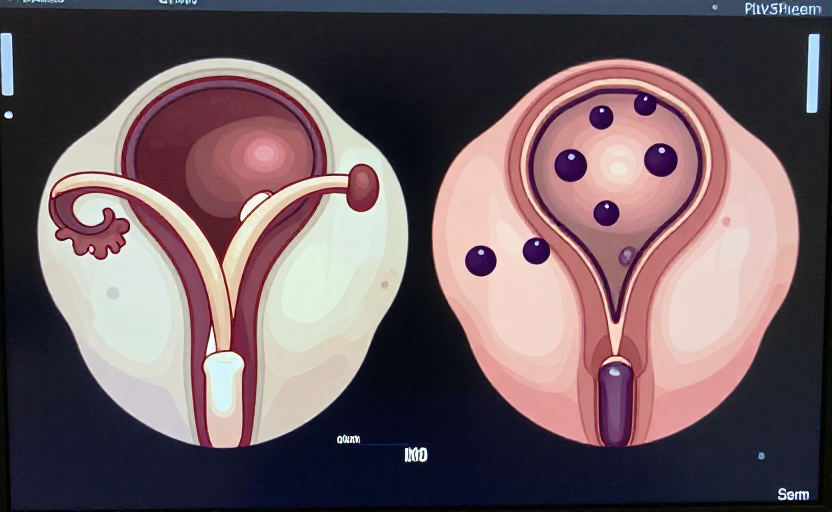
When an endocrinologist orders a pelvic ultrasound for suspected PCOS, they are evaluating specific criteria. The classic finding isn’t large, painful cysts, but rather a high number of very small, immature follicles that have not progressed to ovulation. This appearance is often described as ‘polycystic ovaries’ or a ‘string of pearls.’
The formal diagnostic criteria, often called the Rotterdam criteria, require at least two of three features: irregular ovulation, signs of high androgen levels (like excess hair growth or acne), and the polycystic ovarian morphology on ultrasound. For the ultrasound finding specifically, this typically means seeing 20 or more follicles measuring 2-9 mm in diameter in one or both ovaries, and/or an increased ovarian volume. It’s a count of follicles, not true cysts.
The ultrasound in PCOS is capturing a snapshot of stalled development—many follicles started but none completed the journey to release an egg.
Differentiating PCOS follicles from other ovarian cysts
This is a critical point of understanding. The ‘cysts’ in PCOS are usually antral follicles—small, fluid-filled sacs that each contain an immature egg. They are a normal part of the menstrual cycle; in PCOS, there are simply many more of them due to hormonal signals.
These differ significantly from other types of ovarian cysts that may cause concern:
- Functional Cysts (Corpus Luteum or Follicular Cysts): These develop as part of a normal cycle and usually resolve on their own within a few weeks.
- Dermoid Cysts or Cystadenomas: These are benign growths with different origins and structures, not related to the follicle count of PCOS.
- Endometriomas (‘Chocolate Cysts’): These are associated with endometriosis, not PCOS.
An endocrinologist is skilled at distinguishing this polycystic morphology from these other structures. The context—your symptoms, age, and hormone levels—is essential for accurate interpretation.
The role of monitoring over time
Once PCOS is diagnosed, the need for frequent ultrasound monitoring of the ovaries alone is often low. Routine, repeated ultrasounds are not typically required unless new symptoms arise, such as acute pelvic pain, a rapidly changing pelvic exam, or irregular bleeding that suggests a different issue.
Monitoring in PCOS shifts focus from the ovarian structure to managing the metabolic and hormonal aspects. Your endocrinologist will likely track:
- Symptom changes (menstrual regularity, hirsutism, skin changes)
- Weight and metabolic markers (like blood pressure)
- Periodic blood tests for hormones, glucose, and lipids
This approach prioritizes your overall health risks, such as insulin resistance and cardiovascular health, rather than just the ovarian appearance.
When a cyst in PCOS warrants closer attention
While the many small follicles of PCOS themselves aren’t dangerous, it is still possible for other types of cysts to develop. The key is recognizing symptoms that fall outside the usual PCOS pattern.
You should discuss new or worsening symptoms with your doctor promptly. These include sudden, severe pelvic or abdominal pain, pain accompanied by fever or vomiting, feeling full quickly or bloating, and any unexplained changes in your menstrual bleeding. Such symptoms could indicate a large functional cyst, torsion (twisting of the ovary), or, very rarely, other growths that need evaluation.
Understanding cancer risk
It’s a common worry, but having polycystic ovaries from PCOS does not mean your ovaries are cancerous. The small follicles themselves are not pre-cancerous. However, the chronic lack of ovulation associated with PCOS can lead to prolonged exposure of the uterine lining to estrogen without the balancing effect of progesterone. This can increase the risk of endometrial hyperplasia, a thickening of the uterine lining that, if unchecked over many years, could increase the risk of endometrial cancer. This is why managing cycles and ensuring the lining is shed regularly is a key part of PCOS care.
How treatment can change the picture
Effective management of PCOS can actually alter the ovarian ultrasound findings over time. Interventions that improve hormonal balance often reduce the number of visible small follicles.
- Lifestyle Approaches: Nutrition and exercise that improve insulin sensitivity can help restore more regular ovulation, potentially changing ovarian morphology.
- Hormonal Birth Control: The pill, patch, or ring suppresses the hormonal signals that cause multiple follicles to develop. On ultrasound, the ovaries often appear quieter, with fewer small follicles.
- Ovulation-Induction Medications: For those trying to conceive, drugs like letrozole or clomiphene citrate aim to stimulate one dominant follicle to grow and ovulate, temporarily shifting the polycystic pattern.
Seeing these changes on a follow-up ultrasound can be a positive sign that the treatment is addressing the underlying hormonal drivers.
The journey with PCOS is long-term, and understanding what your doctor is evaluating—and why—can empower you to be an active participant in your care. The focus evolves from initial diagnosis toward sustainable management of your whole health, with the ovaries being one piece of a much larger puzzle.









