
If you’ve ever heard the term ‘ovarian cyst’ and felt a wave of concern, you’re not alone. The phrase can sound alarming, conjuring images of a serious health issue. But in reality, ovarian cysts are incredibly common—most women will develop at least one in their lifetime—and the vast majority are harmless, resolving on their own without you ever knowing they were there. The key is understanding the difference between a normal, functional part of the menstrual cycle and a cyst that may need a closer look, especially in the context of a condition like Polycystic Ovary Syndrome (PCOS).
This guide walks through the practical details: what ovarian cysts actually are, the different types you might encounter, the symptoms that warrant attention, and how PCOS fits into the picture. It’s meant to demystify, not diagnose, and to provide a clear foundation for conversations with your healthcare provider.
What exactly is an ovarian cyst?
At its simplest, an ovarian cyst is a fluid-filled sac that forms on or inside an ovary. Think of your ovaries as small, almond-shaped organs that have two main jobs: releasing an egg each month (ovulation) and producing the hormones estrogen and progesterone. Cysts are often a natural byproduct of this monthly cycle.
During a typical cycle, follicles—tiny sacs in the ovaries—mature and eventually release an egg. Sometimes, this process doesn’t go exactly as planned. A follicle might keep growing instead of releasing its egg, or the sac that remains after ovulation (the corpus luteum) might fill with fluid. These are called functional cysts, and they’re the most common type. They’re usually a sign your ovaries are doing their job, even if a little irregularly, and they typically disappear within one to three menstrual cycles.
Types of ovarian cysts beyond the functional
While functional cysts are par for the course, other types can develop. Knowing the names and basic characteristics helps in understanding what a doctor might be looking for during an exam or ultrasound.
Dermoid cysts are strange but usually benign. They form from embryonic cells and can contain tissue like hair, skin, or even teeth. Cystadenomas develop on the surface of the ovary and can be filled with a watery or mucous-like fluid. They can grow quite large but are typically non-cancerous.
Then there are endometriomas, sometimes called ‘chocolate cysts.’ These form when tissue similar to the uterine lining (endometrium) grows on the ovaries. They fill with old, dark blood and are associated with endometriosis, a condition that can cause significant pelvic pain and fertility challenges.
The term ‘cyst’ simply describes a sac of fluid. It does not automatically mean cancer. In fact, ovarian cysts are very rarely cancerous, especially in premenopausal women.
When do cysts cause symptoms?
Many cysts are silent passengers. You might only discover one incidentally during a routine pelvic exam or an ultrasound for another reason. Symptoms tend to arise if a cyst grows large, ruptures, or twists (a painful event called ovarian torsion).
Pay attention to your body. Symptoms that suggest a cyst may need evaluation include:
- A dull ache or sharp pain in the lower abdomen, often on one side
- Feeling of fullness, pressure, or bloating in the abdomen
- Pain during intercourse or bowel movements
- Changes in your menstrual cycle, such as irregular periods or spotting
- A frequent need to urinate, if a cyst is pressing on the bladder
Sudden, severe abdominal pain, especially with fever, dizziness, or rapid breathing, requires immediate medical attention, as it could signal a ruptured cyst or torsion.
Ovarian cysts and PCOS: What’s the connection?
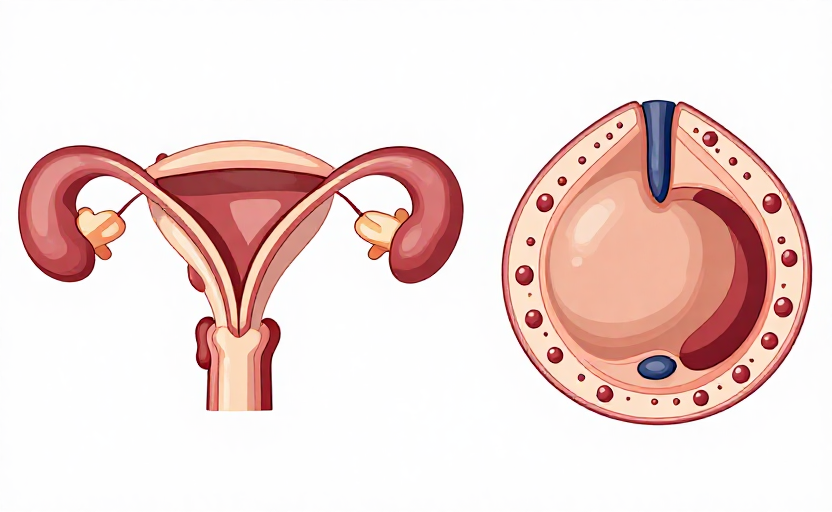
This is where terminology often causes confusion. Polycystic Ovary Syndrome (PCOS) is a hormonal and metabolic condition. The ‘cysts’ in PCOS are not large, problematic cysts like those described above. Instead, they are numerous small, immature follicles that accumulate around the edge of the ovary because ovulation isn’t occurring regularly. On an ultrasound, this can look like a ‘string of pearls.’
PCOS is diagnosed based on a combination of factors, not just the presence of these follicles. The Rotterdam criteria, commonly used for diagnosis, require at least two of these three features: irregular or absent ovulation, clinical or biochemical signs of high androgen levels (like excess facial hair or acne), and the polycystic ovarian morphology on ultrasound.
So, while someone with PCOS has ovaries that may appear ‘polycystic,’ the condition itself is a systemic endocrine disorder with implications for metabolism, fertility, and long-term health. Having a single functional ovarian cyst does not mean you have PCOS.
How are ovarian cysts evaluated and managed?
If you have symptoms or a cyst is found, your doctor’s first step is usually a pelvic ultrasound. This imaging test can reveal the cyst’s size, location, and composition—whether it’s simple (filled with fluid) or complex (having solid areas or separations).
Management is almost always guided by a ‘watch and wait’ philosophy for simple, small cysts, especially in premenopausal women. Your doctor may recommend a follow-up ultrasound in a few months to see if it has resolved. For larger cysts, complex cysts, or those causing significant symptoms, further steps might be discussed.
Treatment, if needed, can range from hormonal birth control to prevent new functional cysts from forming, to laparoscopic surgery to remove a persistent or suspicious cyst while preserving the ovary. The approach is highly individualized, depending on your age, symptoms, and whether you’re hoping to conceive.
Living with and monitoring ovarian health
Awareness is your best tool. Keeping a simple log of your menstrual cycles and any unusual pelvic pain, bloating, or changes can provide valuable clues for you and your doctor. Regular pelvic exams are a cornerstone of preventive care.
For those with PCOS, management focuses on the broader hormonal picture—addressing insulin resistance, regulating cycles, and managing symptoms like excess hair growth. Lifestyle approaches, including balanced nutrition and regular physical activity, are fundamental first-line strategies for overall ovarian and metabolic health.
Remember, the goal isn’t to fear every twinge or blip, but to build a knowledgeable partnership with your healthcare team. Understanding the landscape of ovarian cysts—from the common functional type to the distinct presentation in PCOS—empowers you to ask the right questions and make informed decisions about your well-being.









