For many of us, the word "plaque" conjures up images of a trip to the dentist. But there is another, far more serious type of plaque that can build up silently inside your arteries for decades. This is the stuff behind heart attacks, strokes, and peripheral artery disease. Understanding how it gets there—and what steps you can actually take in response—is one of the most powerful things you can do for your long-term health.
Let’s walk through the process with the clarity a cardiologist would bring to a conversation with a patient. We’ll look at why plaque forms, what it’s made of, and—most importantly—what the research shows about slowing it down or stopping it entirely.
What is arterial plaque, exactly?
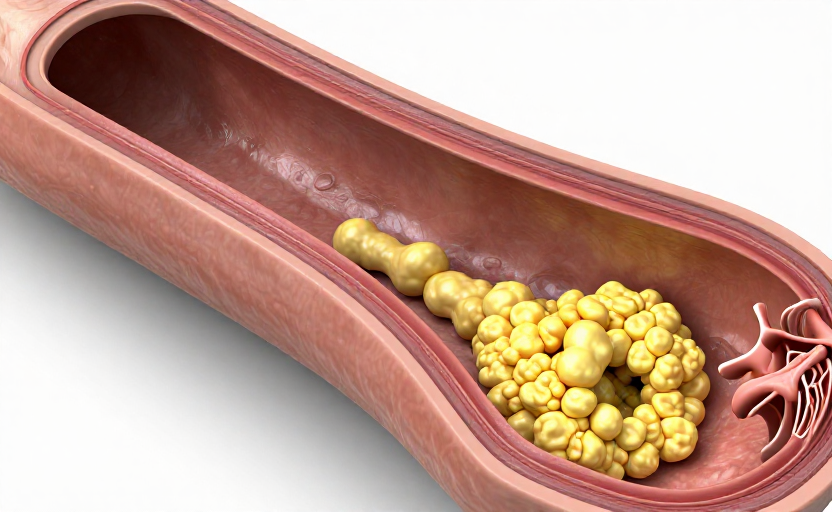
Arterial plaque isn't a single substance. Think of it more like a complex biological wound that is trying to heal in the wrong environment. At its core, plaque is a mix of fats (primarily cholesterol), calcium, cellular waste, and a protein called fibrin that helps with blood clotting. When this mixture accumulates on the inner lining of your arteries—a layer called the endothelium—it forms a hard, waxy deposit.
A healthy artery is smooth and flexible. An artery with plaque is rough, stiff, and narrowed. This narrowing is what doctors call atherosclerosis.
The danger isn't just the narrowing itself. The real threat comes when a plaque becomes unstable. If that cap over the plaque ruptures, your body responds as if it’s a bleeding wound, forming a blood clot over the site. That clot can block blood flow completely in a matter of seconds, causing a heart attack or stroke.
The step-by-step story of how plaque starts
Plaque formation is not a random event. It follows a predictable, stepwise pattern once the conditions are right. Here is how the process unfolds, from the very beginning.
Step 1: Damage to the endothelium
Every artery is lined with a thin, single layer of cells called the endothelium. This lining is incredibly important—it regulates blood pressure, prevents clotting where it isn't needed, and keeps the vessel wall healthy. The problem begins when this lining gets damaged or becomes dysfunctional.
What causes this damage? The usual suspects include high blood pressure (which creates physical stress on the wall), high blood sugar (which is inflammatory), and the chemicals in cigarette smoke. High LDL cholesterol also contributes to endothelial dysfunction even before visible damage occurs.
Step 2: LDL cholesterol enters the wall
Once the endothelium is compromised, it becomes more porous. Low-density lipoprotein (LDL) cholesterol—often labeled the "bad" cholesterol—can now pass from the bloodstream into the artery wall. Once inside, it becomes trapped in the sub-endothelial space, the layer just beneath the lining.
This is a critical tipping point. If LDL levels are high, more particles enter than can leave. The artery wall is now harboring fat where it does not belong.
Step 3: Oxidation triggers inflammation
Inside the artery wall, LDL cholesterol undergoes oxidation. This is a chemical change that makes the LDL particle toxic. The body recognizes this as a threat, and the immune system sends out a distress signal. White blood cells, particularly a type called monocytes, rush to the site. They turn into macrophages, which are essentially cellular garbage trucks designed to eat up the oxidized LDL.
This is where the irony lies. The body's own defense mechanism starts to become the problem. The macrophages gorge themselves on the fatty cholesterol until they become bloated and foam-like. Scientists call them "foam cells." These foam cells accumulate beneath the endothelium, creating the earliest visible stage of plaque: a fatty streak.
Step 4: The smooth muscle cap forms
The artery wall is not defenseless. It tries to contain the damage. Smooth muscle cells from the middle layer of the artery migrate to the site and form a fibrous cap over the growing collection of foam cells and debris. This cap is intended to separate the dangerous contents from the blood flowing above it.
At this point, a plaque is now fully established. It has a soft, fatty core (the necrotic core, filled with dead cells and cholesterol) and a tough fibrous cap on top.
What makes a plaque dangerous (or stable)
Not all plaque is equal. A stable plaque has a thick, strong fibrous cap. It may narrow the artery significantly, but it is less likely to rupture. A vulnerable or unstable plaque has a very thin cap and a large, inflamed core. This is the ticking time bomb.
Inflammation is the key driver here. Chronic inflammation thins the cap and makes it fragile. When that cap ruptures, the contents of the core are exposed to the blood, which triggers an immediate clotting cascade. That final clot is what causes the acute event.
This explains why someone can have relatively mild blockage in their arteries on a stress test but still suffer a major heart attack—the plaque that ruptures wasn't the biggest one, it was simply the most inflamed one.
What you can do about it
Once you understand that plaque is driven by endothelial damage, LDL retention, and inflammation, the strategies for addressing it become clearer. The goal isn't always to "unclog" the arteries (which is very difficult with lifestyle alone), but rather to stabilize the plaque you have and prevent new plaque from forming.
Here are the evidence-backed approaches a cardiologist would typically recommend.
Lower your LDL cholesterol aggressively
You cannot stop the process of plaque formation at the source without addressing LDL particles. If less LDL enters the wall, there is less fuel for the fire. Dietary changes—reducing saturated fat and trans fats, and increasing soluble fiber from oats, beans, and flaxseed—make a measurable difference. For many people, however, diet alone is not enough to get LDL to optimal levels, which is why statins and other cholesterol-lowering medications are so commonly prescribed.
Control inflammation
Since inflammation is what makes a plaque unstable, controlling it is just as important as lowering cholesterol. Regular physical activity, weight management, adequate sleep, and a diet rich in anti-inflammatory compounds (like those found in fatty fish, olive oil, and leafy greens) are foundational. Omega-3 fatty acids, found in fish like salmon and sardines, are particularly helpful here.
Protect the endothelium
The first step of the entire process is damage to the artery lining. Higher blood pressure is a primary cause of that damage. Keeping blood pressure within a healthy range (typically under 130/80 mm Hg, though your doctor will have a specific target for you) is one of the best ways to preserve endothelial health. Reducing sodium intake, managing stress, and staying active all play a role.
Avoiding the accelerators
Smoking and vaping are non-negotiable accelerators of plaque formation. They directly damage the endothelium and promote inflammation. Type 2 diabetes and prediabetes also dramatically speed up the process because high blood sugar is itself inflammatory and damages the artery lining. Managing blood sugar through diet and, if needed, medication is vital.
The reality is that plaque formation is a slow, cumulative process that often begins in young adulthood. The good news is that it is also a process you can powerfully influence. You don't need to be perfect—but consistent action on cholesterol, inflammation, blood pressure, and lifestyle choices will shift the odds dramatically in your favor. Talking to your primary care doctor or a cardiologist about your personal risk factors is the best first step you can take today.