If you live with polycystic ovary syndrome (PCOS), you already know that your menstrual cycle doesn’t always follow the calendar. Periods may arrive late, skip a month (or several), or show up at completely unpredictable intervals. It’s easy to chalk that up as “just how my body works” and move on. But here’s what many people don’t realize: the real story isn’t the irregularity itself—it’s what that irregularity signals about ovulation.
Irregular cycles are the surface symptom. Beneath them, two often-overlooked changes can quietly confirm that ovulation is inconsistent or absent. Recognizing these subtle signs matters whether you are trying to conceive, managing long-term health risks, or simply trying to understand your body better. Let’s look at the two most telling clues and why paying attention to them can change how you approach PCOS.
The first subtle sign: unpredictable cycle length variability
Most people think of “irregular” as simply not having a 28-day cycle. But the real subtlety lies in the variability from month to month. A woman with healthy ovulation might have cycles that range from 26 to 30 days—highly predictable within a tight window. In PCOS, especially when ovulation is being disrupted, cycles may range from 35 days one month to 55 the next, and then suddenly 24 days.
This wide swing is not random. It often reflects anovulatory cycles (where no egg is released) followed by a late ovulatory cycle. Because the body doesn’t ovulate, the usual hormonal feedback loop fails, and the lining of the uterus may build up until it sheds unpredictably. If you track your cycles and notice that the length constantly jumps by two weeks or more, you are likely experiencing sporadic or absent ovulation.
Some people with PCOS also experience what is called “breakthrough bleeding” between actual periods. That spotting or light flow mid-cycle doesn’t always mean ovulation occurred—it can signal unstable estrogen levels caused by a follicle that didn’t mature. Spotting paired with a 50-day gap between full periods is a strong clue that ovulation is not happening regularly.
A quick reality check: If your typical cycle length varies by more than 7–9 days across several months, it’s worth talking to a healthcare provider about whether you are actually ovulating.
The second subtle sign: a missing or inconsistent luteal phase warmth
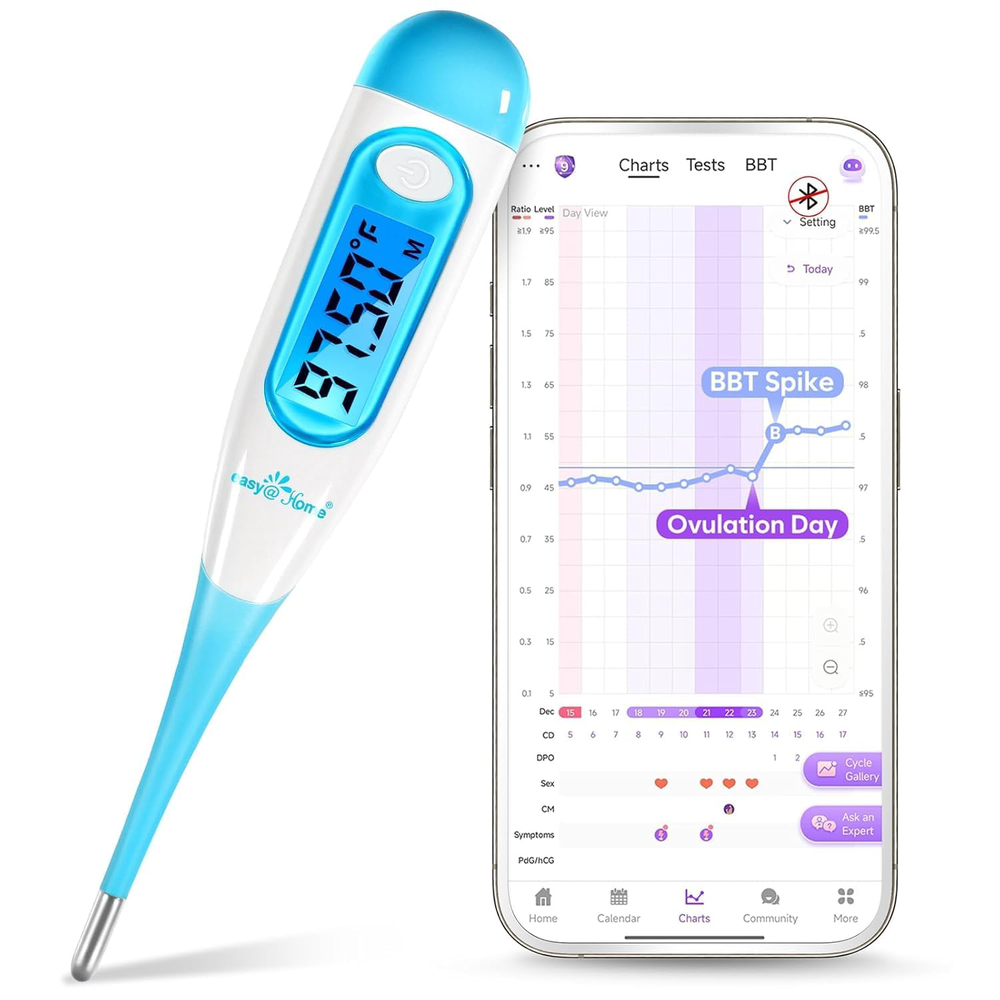
Ovulation triggers a rise in progesterone, which raises your basal body temperature by about 0.5 to 1 degree Fahrenheit. That temperature stays elevated for roughly 10 to 16 days after ovulation—this is known as the luteal phase. For someone with regular ovulation, that shift is clear: cool before ovulation, warmer after, then a drop before the next period.
In PCOS-related anovulation, one of two things happens. Either the temperature never rises (no ovulation at all), or it rises for only a few days before dropping. A very short luteal phase—under 10 days of consistently elevated temperature—is a subtle sign that the body is trying to ovulate but failing to sustain it. You might still get a period, but the ovulation attempt was weak, and progesterone levels stayed too low to prepare the uterine lining properly.
This pattern is especially easy to miss if you aren’t formally charting. Many women with PCOS assume they are ovulating because they get some bleeding each month, but a short luteal phase may mean they are releasing poor-quality eggs or not ovulating at all. The result: reduced fertility and ongoing hormonal imbalance that can affect mood, sleep, and energy.
How to spot this sign without daily temperature tracking
Not everyone wants to wake up and record their basal body temperature, and that’s fine. You can still detect a short or absent luteal phase by paying attention to premenstrual symptoms. A normal luteal phase of 12 to 14 days usually brings noticeable signs like breast tenderness, bloating, mood changes, and food cravings. If these symptoms last only 3 to 6 days before your period starts—or if they change drastically month to month—it suggests that progesterone never fully kicked in. That’s another subtle sign that ovulation might be faulty.
Why these subtle signs matter beyond conception
It is easy to dismiss cycle details when pregnancy is not your immediate goal. But anovulatory cycles don’t just affect fertility—they shape your long-term health. When the uterine lining builds up without regular shedding under progesterone influence, it increases the risk of endometrial hyperplasia. The hormonal instability also feeds insulin resistance, weight gain, and acne, creating a loop that makes PCOS harder to manage.
Recognizing these two signs—wide cycle-length variability and a short or absent thermal shift—gives you specific data to bring to your healthcare provider. Instead of saying “my periods are all over the place,” you can say “my cycles vary from 38 to 60 days and my temperature chart shows only 7 days of elevation.” That precision can lead to better-targeted lab work and treatment strategies, such as checking progesterone levels on day 21 of your cycle (adjusted to your actual timeline) or looking at day 3 follicle-stimulating hormone and estradiol levels.
What you can do about it (without prescriptions)
If these signs resonate with you, the next step is to gather 2–3 months of data. Use a simple paper chart, a period-tracking app, or a basal thermometer if you want deeper insight. Focus on:
- Recording the first day of bleeding and counting the days until the next period.
- Noting any mid-cycle spotting or unusual cramping.
- Observing how many days your premenstrual symptoms last each cycle.
Supportive lifestyle changes—consistent sleep, balanced blood sugar through fiber-rich meals, and stress management—can improve the environment for ovulation over time. But more than anything, the most powerful step is knowing what your cycles are actually doing. The subtle signs of disrupted ovulation are not something you have to decode alone; they are signals your body is already sending. Learning to read them is the first move toward better PCOS management, whether your goal is pregnancy, steady moods, or just feeling more in control.
If you track these signs and consistently see wide variability or short luteal phases, a reproductive endocrinologist or a PCOS-savvy gynecologist can help interpret them in context of your overall health. You don’t need to suffer through the guessing game—your cycles already hold the answers; you just need to know where to look.